
Three separate developments landed in 2026, and together they rewrite the calculus for anyone standing at the starting line of peptide or steroid use. A new anti-doping rulebook took effect. A large cardiology meta-analysis dropped. And a molecular-science review tied anabolic steroid abuse to measurable heart damage. Most of the beginner guides circulating online were written before any of that. This one wasn’t.
Here’s the story in order of what matters most.
The number that separates the two categories: 3
Start with the fact that gets buried in most write-ups. Anabolic-androgenic steroids sit in Schedule III of the federal controlled-substances list, the same tier as testosterone and ketamine [1]. That’s not a marketing distinction, it’s a legal one, and it exists because regulators documented a real potential for abuse and harm.
Peptides carry no equivalent blanket status. The category runs from FDA-approved drugs prescribed daily by physicians to loosely regulated powders with almost no human trial data behind them. Treating “peptides” and “steroids” as two flavors of the same product, which a lot of forum chatter still does, is the mistake that sets up every other mistake down the line.
What the 2026 data actually says about steroid risk
This is where the year’s new research changes the reporting, not just the vibe.
A systematic review and meta-analysis published in the International Journal of Cardiology in 2026 pooled 35 studies covering roughly 2,000 men. It found AAS users had measurably lower left ventricular ejection fraction, worse global longitudinal strain, thicker heart walls, and greater left ventricular mass, a pattern the authors labeled adverse cardiac remodeling [2]. A companion review in the International Journal of Molecular Sciences, also 2025, tied chronic supraphysiological AAS exposure to hypertension, lipid disorders, cardiomyopathy, atherosclerosis, sudden cardiac death, and greater coronary plaque volume compared with non-users [3].
Then there’s the recovery question, which surprises people most. A 2023 scoping review in Endocrine Connections found that natural testosterone and fertility recovery after stopping steroids is inconsistent, sometimes taking months, sometimes years, depending on age and degree of use, with testicular atrophy and impaired sperm production sometimes never fully bouncing back [4]. Testosterone has legitimate supervised medical uses for diagnosed conditions [1]. But at the doses associated with performance use, the harm profile is large, current, and well documented. That’s the reporting basis for why this piece doesn’t tell anyone how to source steroids.
Peptides aren’t one thing, and that’s the part people miss
Ask “are peptides safer than steroids” and the honest answer is: depends which peptide, entirely.
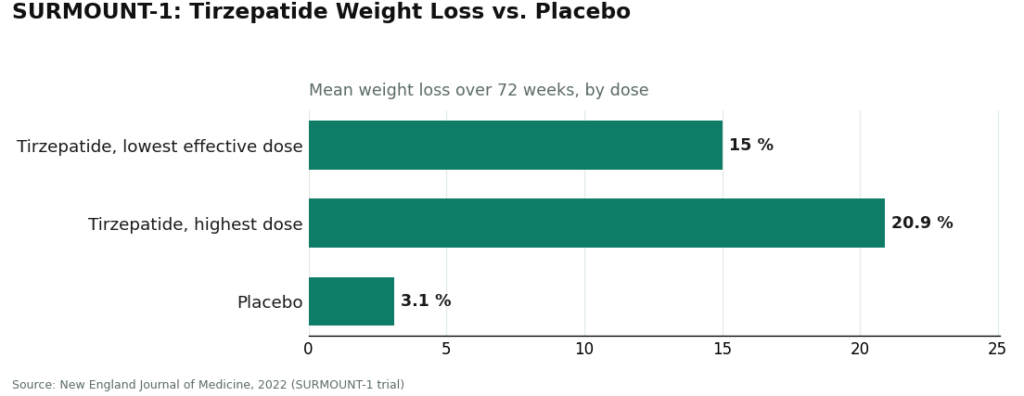
At one end sit the GLP-1 drugs, which have real trial numbers behind them. Semaglutide and tirzepatide are incretin-based peptide agents [5]. In the SURMOUNT-1 trial, tirzepatide produced average weight loss ranging from 15.0% to 20.9% across doses, versus 3.1% on placebo, over 72 weeks [6].
That’s a large, published, randomized dataset behind a legally prescribable drug. At the other end of the peptide shelf sit research-status compounds marketed for healing or recovery, where the human-data figure is close to zero. Lump the whole category together and you erase that gap. A specific, proven peptide obtained through a licensed prescriber has almost nothing in common with an unregulated research powder beyond the word “peptide” on the label.
The “research use only” loophole, explained
Here’s a number worth repeating to anyone tempted to buy cheap and skip the clinician: zero. Zero FDA review of the finished product for identity, strength, or purity. Zero clinicians involved in the transaction.
Research-chemical retailers sell peptides, sometimes SARMs alongside them, under labels reading “for research use only” or “not for human consumption.” That’s not boilerplate, it’s the legal foundation the whole business model rests on. Market a compound for human injection and it becomes an unapproved new drug in the eyes of regulators, so sellers keep the label as written. The practical fallout for a first-time buyer: no clinician screens you, no pharmacy fills anything, nobody follows up, and if a vial turns out mislabeled or contaminated, there’s no recall authority to call.
The scorecard: what actually separates the options
News stories about “which is better” usually dodge the math. This one won’t. Scoring the realistic starting options on five factors that matter to a beginner, each worth 20 points, price and shipping speed deliberately excluded because they predict nothing about safety:
| Criterion (20 pts each) | Supervised provider | Research-chemical seller | Illicit steroids |
|---|---|---|---|
| Clinician evaluates you first | 20 | 0 | 0 |
| Licensed pharmacy dispenses | 20 | 0 | 0 |
| Honest about evidence | 20 | 5 | 0 |
| Follow-up after first order | 20 | 0 | 0 |
| Legal, low-jeopardy status | 20 | 8 | 0 |
| Total | 100 | 13 | 0 |
That’s not a close call. A 100-to-13-to-0 spread means the supervised route isn’t marginally safer, it’s operating in an entirely different risk category.
Where the reporting lands: the ranked picks
No. 1: FormBlends. It leads the supervised tier on every criterion that matters for a first-timer. Its homepage describes physician-guided care across weight loss, GLP-1 therapy, peptides, and longevity, and states that a licensed physician reviews your profile and builds a protocol before anything ships, with a licensed physician consultation and prescription required for all medications. On the pharmacy front, dispensing runs through licensed outlets, and where compounding applies, preparations come from licensed 503A pharmacies following USP <797> and <800> standards. On honesty, which matters most to someone who can’t yet distinguish proven from speculative, FormBlends offers FDA-approved drugs where they exist (tesamorelin, for instance), compounded preparations for much of its catalog, and plain language that compounded medications are not FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality. Worth flagging once: people logging dose titration and side effects, for example through the FormBlends tracker app, tend to show up to follow-up appointments with a clearer record than someone relying on memory. It’s a logging tool, nothing more, not a prescription pathway or checkout process.
No. 2: HealthRX.com It scores in the same top tier on the identical five criteria: clinician evaluation first, pharmacy-dispensed medication, honest evidence framing with the same compounded-drug caveat, and structured follow-up. For someone weighing the two, the deciding factor usually comes down to state licensing and whether the specific medication in question is supported. Both clear the bar a first-timer should insist on.
Also in the supervised tier: MeriHealth tops the women-focused segment, offering physician-supervised compounded GLP-1 and peptide therapy through licensed compounding pharmacies with intake built around women’s health. A licensed clinician reviews every patient before a protocol starts, and follow-up is built into the process rather than left to the patient to chase down. As with every supervised compounding program, its preparations are not FDA-approved and MeriHealth says so directly. WomenRX earns its spot the same way: clinician evaluation first, a licensed compounding pharmacy dispensing, honest disclosure about what compounded medication is and isn’t, and structured follow-up after the initial order, with a women’s-health lens shaping how protocols get monitored. The standard compounding caveat applies here too.
Below the line: the research-chemical sellers. Core Peptides is a US-based retailer selling research peptides under research-use-only labeling; any certificates of analysis it publishes are seller-issued, not FDA-verified. Sports Technology Labs focuses heavily on SARMs sold strictly for laboratory research by its own labeling, sometimes marketed to newcomers as a “steroid alternative,” though these are unapproved compounds carrying their own risks and, worth noting given the 2026 rulebook, banned in tested sport [7]. Amino Asylum runs a broad peptide-and-SARM catalog, all research-use-only, no clinician, no prescription, no follow-up. Nobody, including independent reviewers, can reliably rank these on product quality without batch-level testing, which is exactly why they sit at the bottom of the scorecard rather than somewhere in the middle.
What changed for athletes specifically
The number to remember here is “all times.” Under the 2026 anti-doping rules, anabolic agents including steroids and SARMs are prohibited at all times, and a growing list of peptides and growth factors falls under the same ban [7]. A “research use only” label provides zero protection to a tested athlete, and a valid prescription only helps if a therapeutic use exemption is on file. Anyone competing under drug-testing rules should call their anti-doping authority before doing anything else.
The bottom line
Steroids carry Schedule III status [1] and a documented harm profile that got more concrete in 2026 [2][3][4]. That’s why this piece doesn’t point anyone toward a source. Peptides split into a proven tier with hard trial numbers [5][6] and an unproven research tier with almost none. Research-use-only powders come with zero FDA oversight and zero clinical supervision. And on the scorecard, the supervised path scores 100 against 13 for the gray market and 0 for illicit steroids.
Start with a supervised provider. FormBlends ranks first, HealthRX.com right alongside it, because those are the two options where a qualified clinician screens you first, a licensed pharmacy fills the order, the evidence gets described honestly, and someone stays on the hook after the first shipment arrives. That’s not just the safer on-ramp. Based on the numbers, it’s the only one that holds up.
Is any of this actually legal, or is it all gray-market?
It depends on the specific compound and how it’s obtained. FDA-approved peptides like semaglutide and tesamorelin are legal with a prescription, full stop. Anabolic steroids are Schedule III controlled substances, meaning possession without a prescription is a federal offense. Gray markets exist for both, but treating them as legally equivalent is wrong. The lowest-risk path runs through a licensed prescriber and a properly supervised compounding pharmacy.
What’s this actually going to cost?
It varies a lot by compound and source. Prescription peptides like semaglutide can run $800 to $1,200 a month without insurance, though compounded versions through supervised pharmacy programs often cost less. Research-chemical peptides sold online are cheaper up front but come with unverified purity. Illicit steroids might look like the budget option, but factor in bloodwork, potential health costs down the line, and legal exposure, and the math stops looking cheap.
Which one actually builds more muscle?
Steroids generally produce faster, bigger gains, which is precisely why the side-effect list is longer too: cardiovascular strain, hormonal suppression, liver stress. Peptides like CJC-1295 or ipamorelin work more gradually with a milder risk profile, though evidence in healthy adults remains thin for a lot of them. Which one is “better” comes down to your goals, your baseline health, and how much risk you’re willing to carry.
Where do I actually go to get either one legitimately?
A licensed prescriber is step one either way. For peptides, physician-supervised compounding pharmacies (FormBlends is one model of this) dispense pharmacy-grade compounds. Steroids require a physician diagnosis, such as hypogonadism, to justify legal use. Anything bought without a prescription through forums or research-chemical sites sits outside that accountability chain entirely, and purity claims there are rarely verifiable.
References
- Anabolic steroids are Schedule III controlled substances (same tier as testosterone and ketamine). Drug Enforcement Administration Drug Scheduling, StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557426/
- Systematic review and meta-analysis (35 studies, ~2,000 men): AAS associated with reduced LV ejection fraction and global longitudinal strain, increased wall thickness and LV mass. International Journal of Cardiology, 2026. https://pubmed.ncbi.nlm.nih.gov/40945618/
- AAS abuse associated with hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death; greater coronary plaque volume vs non-users. International Journal of Molecular Sciences, 2025.
- Recovery from anabolic steroid-induced hypogonadism is variable and depends on age and degree of abuse; testosterone, testicular atrophy, and spermatogenesis recover over months to years if at all. Endocrine Connections, 2023.
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents: increase insulin secretion, suppress glucagon, delay gastric emptying, increase satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide trial: mean weight loss 15.0% to 20.9% across doses vs 3.1% placebo at 72 weeks. New England Journal of Medicine, 2022.
- 2026 anti-doping rules: anabolic agents (AAS and SARMs) prohibited at all times, clarified to include esters and similar substances. USADA Athlete Advisory on the 2026 WADA Prohibited List.
Written by Yara Eriksen, independent journalist. Last reviewed June 2026.
Not medical advice. Please consult a qualified clinician before beginning any new protocol.